IRANDERMA |
|
Quiz: January 2005 |
A 6-year-old boy presented with grouped papulovesicular eruptions on his flank since months ago. Medical history was significant for a surgery performed in neonatal period for a cystic mass (?) in this area.
What is your diagnosis?
What do you recommend in managing this patient?


Diagnosis: lymphangioma circumscriptum
Comment by; M. Mehravaran, MD, Dermatologist/ Szeged, Hungary:
Lymphatic malformations present as localized or diffuse malformations of the lymphatic vessels. Solitary lymphatic cysts, so called cystic hygromas are most common on the neck. They are fluid filled and frequently communicate with adjacent lymphatic structures. Localized multicystic lymphatic malformations of the skin and mucosa, so-called lymphangioma circumscriptum, present as clusters of clear, fluid-filled vesicles that often become discolored by bleeding from surrounding capillaries. These lesions often have deeper components not initially evident, but that become apparent if the lesion recurs after an incomplete excision. Excessive lymphatic malformations usually present with lymphedema of the affected area, often in association with more superficial vesicular skin lesions. In some cases, deeper connective tissues and viscera may be affected. Severe complications, including recurrent leakage of lymph, recurrent cellulitis, and cosmetic disfigurement, can occur.
Clinically, there are three basic types of lymphangioma, which are differentiated by size. Solitary simple lymphangiomas are uncommon and present in infancy as nondescript dermal or subcutaneous nodules. Lymphangioma circumscriptum consists of multiple clustered small vesicles, classically described as resembling frog spawn. Cavernous lymphangiomas (cystic hygromas) are large, ill defined masses of dilated csystic lymphatics, which may underlie areas of the more superficial lymphangioma circumscriptum.
Lymphangioma usually appear in infancy, and most are present by the age of 5 year. The sites most commonly involved are neck, axillae, breasts, cheat, buttocks and thights. Lymphangioma circumscriptum, as seen here, a few of the thick, tense vesicles will have a component of heme pigmentation. Recurrenc after excision (note the linear scars) is common (as seen in this case report too), probably because of an unrecognized deep lymphangioma component.
lymphangioma circumscriptum:
Lymphangioma circumscriptum is an uncommon hamartomatous malformation that is not only localized to an area of skin, but also spreads to subcutaneous tissue and muscle (Whimster's hypothesis).
LC may present at any age but is usually noted at birth or appear during childhood. The commonest sites are abdomen, axillaryfolds, shoulders, flanks, proximal parts of limbs, the mouth, particularly the tongue and pernium. It manifests with fluid-filled vesicles, which are mostly translucent but may vary in color from red to blue-black well defined, and discrete or grouped resembling frogspawn.
Differential Dx: acquired lymphangioma, angikeratoma, hemangioma
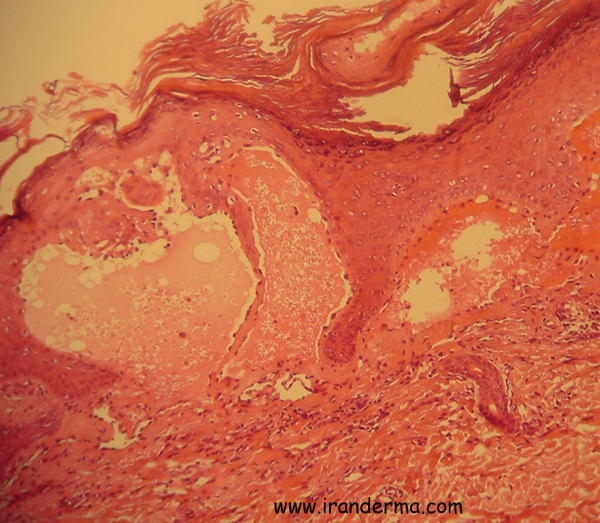
Histology:
Lymphatic malformations feature dilated, thin-walled vessels whose lumens contain frothy appearing proteinaceous material, and are devoid of erythrocytes unless the lesion has been traumatized. These vessels are dispersed throughout the superficial and deep dermis, and subcutis. Delicates valves are present in some vessels. Collections of small lymphocytes are sometimes seen in the adjacent dermis. Deep vessels can be partially surrounded by fascicles of smooth muscle. In lymphangioma ciscumscriptum, round, dilated lymphatic vessels are present just beneath a hyperplastic and hyperkeratotic epidermis.
Treatment:
There is no specific treatment for lymphangiomas. Excisional or laser surgery may be satisfactory for small lesions, but with large lesions surgery is often incomplete and the recurrence rate is high.
Surgical management: small lesions, less than 7 cm diameter, in favourable sites of the body, which are potentially curable; and large lesions, greater than 7 cm diameter on the skin with an even larger area of subcutaneous cysts, in which complete excision of all the skin and subcutaneous vesicles would require skin grafting.
Lasers Therapy:
Carbon dioxide laser vaporization may be a useful alternative to frequently unsuccessful traditional surgical forms of therapy for selective cases of classical lymphangioma circumscriptum.
Because of deeper components, lesions may recur following any surgical technique, including laser ablation, electrosurgery, cryotherapy, and superficial excision. Some lymphatic malformations with a capillary or venous component may be susceptible to continuous-wave light sources that are absorbed well by vascular tissue. Under these ciscumstances, the argon, copper vapor, continuous-wave dye, krypton, and KTP lasers may be of benefit.
In cases with diffuse lymphatic malformations, support garments may be helpful in avoiding progressive lymphangiectasia. Prophylactic antibiotics may also help if recurrent infection becomes a problem.
Acquired
lymphangiectasis is a dilatation of lymphatic vessels that can
result as a complication of surgical intervention and radiation
therapy for malignancy. Acquired lymphangiectasis shares clinical
and histological features with the congenital lesion, lymphangioma
circumscriptum. Diagnosis and treatment of these vesiculobullous
lesions is important because they may be associated with pain,
chronic drainage, and cellulitis.
Acquired
lymphangiectasis (AL) represent superficial lymphatic dilatation
caused by a wide range of scarring processes and occurs as a
consequence of lymphatic damage by an external cause, leading to
obstruction of local lymphatic drainage. It has been reported after
treatment of breast, vulva, cervix, skin, and lung cancers and it is
sometimes termed acquired lymphangiomas . This condition has
also been associated with metastatic lymph node invasion and
obstruction, scleroderma, and scrofuloderma. Acquired lymphangiomas
most commonly occur in adults as a late sequel of mastectomy and
radiation therapy. Patients usually present with numerous
translucent vesicles in a chronic lymphedematous area several years
after surgery with or without radiation therapy.
Fatemeh Jebraeili,MD, Internal Medicine, State University of New York
ايران درما |