IRANDERMA |
|
Quiz: June 2005 |
A 45-year-old male presented with a 2-3 years history for an asymptomatic lesion on the back. He was on no medications and had not any significant medical problem.
What is your diagnosis?

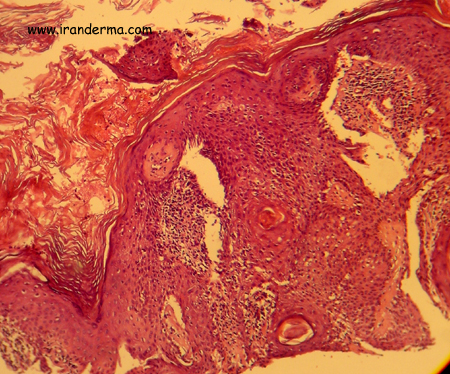
Diagnosis: Seborrheic Keratosis (irritated type)
Seborrheic keratosis (SK) are macular or papular lesions that vary in
color from waxy yellow to dark brown. They most commonly have a velvety or
verrucous surface but may also be flat. A greasy, hyperkeratotic scale is
frequently seen overlying the lesions and is a helpful diagnostic clue in
differntionating these lesions from other pigmented neoplasms. SK may
occur in any anatomic location and vary in size from 1 mm to several
centimeters.
SK are the most common cutaneous neoplasms. They occur in the majority
of elderly caucasian patients but
are not limited to this population. SK are unusual in childhood and increase
in number and size with progressive age. They are most commonly
asymptomatic, though occasional lesions are pruritic. The major concern is
one of cosmesis, and occational confusion with more worrisome pigmented
lesions such as malignant melanoma..
SK are a component of the leser-Trélat
syndrome. In this conditions, the rapid onset of multiple,
pruritic seborrheic keratoses has been associated
with the development of GI malignancy, leukemias, and lymphomas.
Histology:
Generally there is epidermal thikening, the prodominant cell
being rather like the normal basal epidermal cell. Surmounting the
thickened epidermis there is a warty hyperkeratosis whose
arrangment have been linkened to a series of church spires. Within the
lesion are foci of keratinization and horn cysts.
SK have several charatcteristic histologic appearances. Common to all forms is a proliferations of basaloid keratinocytes that have ovoid nuclei, without prominent nucleoli, small amounts of cytoplasm, and variable amounts of melanin. The is no cytologic atypia seen. One characteristic histologic feature of SK is the „horn pseudocyst”. These are crypts lines by keratinocytes containing keratohyaline granules. As these invaginations have irregular shapes, cross-sectioning renders a cystic appearance to their profiles. Pseudocysts contain laminated or basket weave keratin.
Lever's Histopathology of the skin:
In
the irritated, or activated, type of SK, squamous cells outnumber basaloid
cells. The characteristic feature is the presence of numerous whorls or
eddies composed of eosinophilic flattened squamous cells arranged in an
onion-peel fashion, resembling poorly differentiated horn pearls. These
"squamous eddies" are easily differentiated from the horn pearls
of SCC by their large number, small size, and circumscribed configuration.
Treatment:
Chemical peeling, Cryosurgery, Save and Curettage, CO2 laser
vaporization and more recently PDT methods are also growing.
By:
Dr. Mehrdad Mehravaran, Szeged-Hungary
![]()
ايران درما |